 Mahesh Vidula is a member of the MIT Class of 2011 majoring in Biological Engineering. He was born and raised in Chicago, Illinois . In high school and at MIT, Mahesh developed an interest in scientific research and public health. He hopes that making information about scientific issues more available to the general public will increase awareness and encourage action.
Mahesh Vidula is a member of the MIT Class of 2011 majoring in Biological Engineering. He was born and raised in Chicago, Illinois . In high school and at MIT, Mahesh developed an interest in scientific research and public health. He hopes that making information about scientific issues more available to the general public will increase awareness and encourage action. Tuberculosis: Curable, Yet Still A Major Public Health Issue
by Mahesh Vidula
Tuberculosis causes at least 1.7 million deaths around the world per year, and currently ranks as the fourth most deadly infectious disease. An infected host spreads the Mycobacterium tuberculosis (M.tuberculosis) bacteria through aerosolized droplets while coughing or sneezing (Glickman and Jacobs 2001). Since tuberculosis possesses the ability to spread through the air to virtually anyone, the World Health Organization (WHO) has increased its efforts to fight tuberculosis and plans to eradicate the disease by 2050.
M. tuberculosis makes effective use of the immune system to infect the human body. When a host inhales the bacilli, a majority of the bacteria become trapped in the sticky mucosal cells and subsequently removed from the body, while other bacilli pass through to the alveoli (Kasper et al. 2005). Here, the bacteria are engulfed by non-specific, alveolar macrophages and use this opportunity to multiply in the phagosome (Grosset 2003). M. tuberculosis survive in the macrophage due to their ability to retain a tryptophan aspartate-containing coat protein (TACO) that resists the delivery of the bacteria to the lysosome (Pieters 2001). The bacteria eventually destroy the macrophage, only to be engulfed by other macrophages that transport the bacteria to the lymph node (Grosset 2003).
Once in the lymph node, the antigen moves to the cell surface on a major histocompatibility complex class II molecule (Schluger and Rom 1998). The T-cell receptor on the antigen-specific CD4 cells recognizes the peptide on the surface of the macrophage, and the CD4 cells release lymphokines to alert B-cells and killer T-cells of the infection (Schluger and Rom 1998). To fight the bacteria, a cell-mediated immune response is launched; this response consists of antigen-specific T-lymphocytes that fight the bacteria (Grosset 2003).
A granuloma, also known as a tubercle, is created when the antigen-specific CD4 cells, natural killer (NK) cells, B cells, CD8 cells, and activated macrophages surround M. tuberculosis to prevent further spread of the bacteria (Figure 1, Flynn 2004). Activated T-lymphocytes attack the infected macrophages and destroy the surrounding tissue to prevent further bacterial growth during a stage known as caseous necrosis (Grosset 2003). After the initial attack, the center of the tubercle solidifies with some bacteria still inside (Grosset 2003). However, the surviving bacteria are latent since they cannot reproduce due to the low oxygen and pH levels of the tubercle. (Grosset 2003).
In 10% of infected hosts, the center of the tubercle liquefies via an unknown mechanism, and the bacteria spread over the bronchial tree of the lungs (Grosset 2003). The bacteria can now thrive and reproduce in the sufficient oxygen levels, and the host officially has tuberculosis disease. Whenever the infected host coughs, the bacteria spread to the bronchi and other parts of the lungs and body (Grosset 2003). A lung cavity also forms when the tubercle liquefies and drains out (Grosset 2003). Since the cavity cannot heal spontaneously or without treatment, the bacteria spread throughout the lung, and the cell-mediated immune response follows (Grosset 2003). The continued destruction of tissue by the T-lymphocytes forms several cavities and ultimately leads to death.
In 10% of infected hosts, the center of the tubercle liquefies via an unknown mechanism, and the bacteria spread over the bronchial tree of the lungs The bacteria can now thrive and reproduce in the sufficient oxygen levels, and the host officially has tuberculosis disease.
To treat tuberculosis, patients must employ several drugs for around six months. The first line of tuberculosis drugs consists of isoniazid, rifampin, ethambutol, and pyrazinamide (Sahbazian and Weis 2005). While isoniazid begins by obstructing M. tuberculosis cell wall synthesis, rifampin works to impede RNA synthesis in M. tuberculosis, which slows the growth rate of the bacteria (Sahbazian and Weis 2005). Similar to isoniazid, ethambutol also inhibits cell wall synthesis. However, along with pyrazinamide, ethambutol also plays a role in protecting against drug resistance (Sahbazian and Weis 2005). Second line drugs, while not commonly used, include fluoroquinolones, kanamycin, amikacin, and capreomycin. Children and adults follow the same treatments. However, patients with specific diseases must follow different regimens. Specifically, pyrazinamide is not recommended for people with liver disease, while amikacin and capreomycin should be used with caution in kidney disease patients (Irwin and Rippe 2007). In epileptic patients, isoniazid increases seizures; rifampin has been shown to interact dangerously with anti-epileptic drugs (Mayo Clinic). Physicians should always take a proper history before prescribing treatments for tuberculosis patients.
Despite the pharmaceuticals developed by researchers to fight tuberculosis, the disease is on the rise due to drug resistance. If patients fail to follow the medication regimen set by their physicians, the bacteria can become resistant to all four first-line and second-line drugs. Most cases of drug resistance emerge in countries without the resources to provide expensive tuberculosis medications, such as China and countries of the former Soviet Union (Iseman and Heifets 2006). Depending on the case, drug-resistant tuberculosis can be fought using different treatment regimens, including chemotherapy. Moreover, recent research indicates that the combination of meropenem and clavulanate can kill drug resistant strains in vitro, but further studies must be performed in vivo.
Currently, the World Health Organization estimates that among the two billion people worldwide who carry M. tuberculosis, 1 in 10 will develop the disease. These statistics confirm that tuberculosis is a global health issue demanding serious action. It is clear that scientists have carefully studied the biological pathways and revealed the infectious mechanisms to develop powerful treatments. However, due to socioeconomic circumstances, these treatments are not effective and often give rise to drug resistance. While more research directed towards developing advanced treatments can be helpful in curtailing drug-resistant tuberculosis, funding to deliver these medicines to every city, town, and village around the world will save many more lives. Education to ensure that patients follow treatment regimens will make certain that the medicines are effective. Although the global finance crisis may stymie current anti-TB efforts, with greater distribution of resources and education, the World Health Organization goal of eradicating tuberculosis by 2050 can be met.
________________________________________________APPENDIX
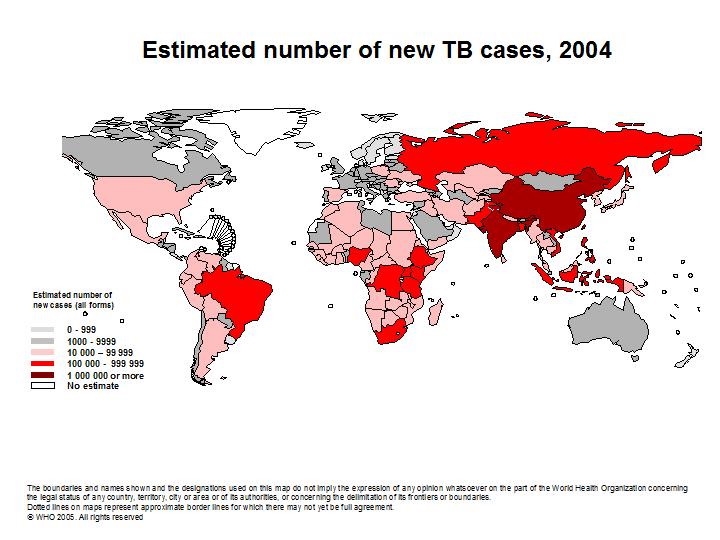 Credit: World Health Organization
Credit: World Health Organization
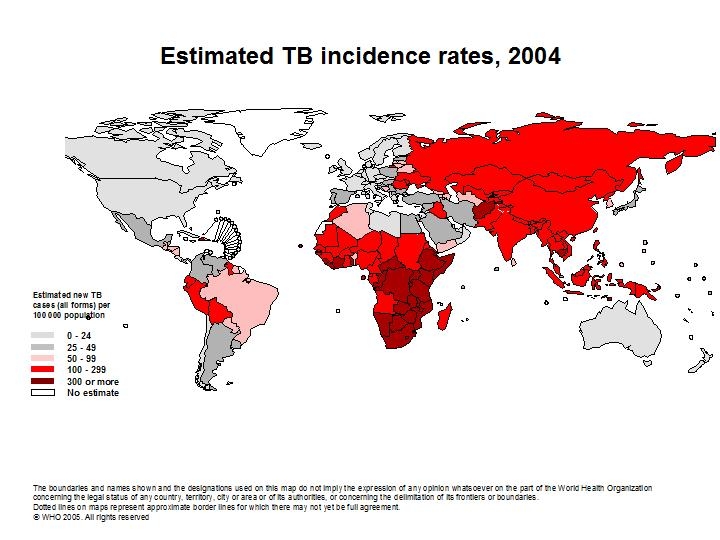 Credit: World Health Organization
Credit: World Health Organization
Global Incidence of TB
Graph of global incidence of tuberculosis until 2004. Credit: World Health Organization. 2006
_______________________________________
Works Cited
(2004), 84(1-2): 93-101.
Glickman, M.S. and W.R. Jacobs, Jr. Microbial Pathogenesis of Mycobacterium tuberculosis:
Dawn of a Discipline. Cell (2001), 104(4): 477-85.
Grosset, J. Mycobacterium tuberculosis in the Extracellular Compartment: an Underestimated
Adversary. Antimicrobial Agents and Chemotherapy (2001), 47(3): 833-836.Irwin, Richard S., and James M. Rippe. Irwin and Rippe's Intensive Care Medicine. 6th ed.
Lippincott Williams & Wilkins, 2007. Google Books. http://books.google.com/books?id=ooH1nH81_h4C
Iseman, M.D. and Heifets, L.B. Rapid detection of tuberculosis and drug-resistant tuberculosis.
NEJM (2006), 355(15): 1606-8.
Joklik, W.K., H.P. Willett, and D.B. Amos. Zinseer Microbiology. 1984. Appleton-Century-
Crofts. Norwalk, Connecticut, p.100-2, 547-63.
Kasper, D. L., E. Braunwald, A.S. Fauci, S. L. Hauser, D. L. Longo, L. Jameson, and K.J.
Isselbacher. “Tuberculosis.” Harrison's Principles of Internal Medicine. 2004. Sixteenth Edition. The McGraw Hill Companies, Inc. Chapter 150.
Lite, Jordan. "Med disables drug-resistant tuberculosis in lab. Will it work in humans?"
26 Feb. 2009. Scientific American.
http://www.sciam.com/blog/60-second-science/post.cfm?id=med-disables-drug-resistant-tubercu-2009-02-26
Pieters, J. Entry and Survival of Pathogenic Mycobacteria in Macrophages. Microbes and
Infection (2001), 3(3): 249-55.
"Rifampin and Isoniazid (Oral Route)." 1 Mar. 2009. Mayo Clinic. 18 Mar. 2009
http://www.mayoclinic.com/health/drug-information/DR600353
Sahbazian, B. and S. Weis. Treatment of Active Tuberculosis: Challenges and Prospects.
Clinics in Chest Medicine (2005), 26 (2): 273-82.
Schluger N.W. and W.N. Rom. The Host Immune Response to Tuberculosis.
American Journal of Respiratory and Critical Care Medicine (1998), 157(3): 679-691.
"Tuberculosis." World Health Organization. http://www.who.int/topics/tuberculosis/en/
"Viral Hepatitis." Medscape.
http://www.medscape.com/content/2003/00/45/79/457918/457918_fig.html