Breast
The current clinical standard for breast cancer detection and diagnosis is screening procedures such as palpation, X-ray mammography, or ultrasound, following by breast biopsy and surgical procedures.X-ray mammography which is essential part in diagnosis of breast cancer do not accurately identify malignant tissue. Because of low specificity of mammography, a high percentage of suspected abnormal lesions (70-90%) are found to be normal or benign upon biopsy, resulting in patient trauma, and increase in cost associated with unnecessary procedures, as well time delay in order to obtain histopathological diagnosis. Our goal is to develop optical spectroscopy techniques to diagnose benign and malignant breast lesions in real-time in a minimally-invasive fashion during breast biopsy and to assist status of margins of resection during breast cancer surgery. We have developed a contact- probe based clinical portqable instrument that is capable of collection Raman, reflectance and fluorescence spectroscopy data in real time. These spectroscopic techniques provide complementary information about tissue biochemical composition. Raman spectroscopy provides specific information about the chemical composition of tissue and are fit using a linear combination of Raman active tissue components (calcium, collagen, lipids, cell cytoplasm, etc.). Diffuse reflectance spectroscopy (DRS) provides information about tissue absorbers (hemoglobin, b-carotene, etc ) and scatterers and are modeled using diffusion theory. Intrinsic fluorescence spectroscopy (IFS) provide information about tissue fluorophores (collagen, NADH, etc.) and is extracted from the combined fluorescence and DRS spectra. The analysis of the data is based on the physical meaningful parameters.
We had conducted several ex vivo and in vivo clinical study at the University Hospitals-Case Medical Center (UH-CMC) at Cleveland, OH. The protocol was approved by the UHC Institutional Review Boards (IRB), as well as the Committee On the Use of Humans as Experimental Subjects (COUHES) of the Massachusetts Institute of Technology. Spectra were collected from fresh breast surgical specimens within 30 minutes after excisional biopsy and lumpectomy or mastectomy procedures. Most of the 30 minute delay was due to gross examination, inking and sectioning of the specimen performed as part of the routine pathology intraoperative consultation. For each surgical specimen reflectance, fluorescence and Raman spectra were collected via optical fiber probe that is brought in gentle contact with the tissue site of interest identified by the pathologist. The entire acquisition time was approximately 5 seconds: each measurement consisted of Raman spectra (830 nm excitation), white light reflectance spectra (300-800nm emission), and fluorescence spectra (340nm excitation).
|
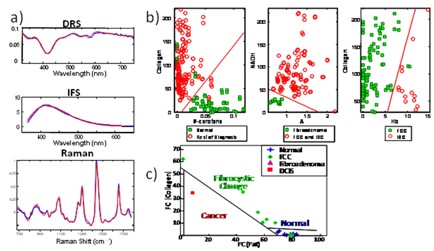
Figure 1. Results of breast clinical studies: a) example of DRS, IFS and Raman spectra (blue – data, red – fit); b) DRS/IFS step-wise diagnostic algorithm; c) Raman diagnostic algorithm for separation normal, fibrocystic change (FCC), fibroadenoma, and infiltrating ductal carcinoma (IDC) |
The interrogated site was subsequently inked and evaluated by histopathologist. Histopathological diagnoses, i.e. normal, fibrocystic change, fibroadenoma, infiltrating ductal carcinoma, etc, were provided by the experienced breast pathologist blinded to the spectroscopic results. Physically meaningful parameters were extracted from spectroscopic information of Raman, IFS and DRS data and correlated to histopathology diagnosis. Previously we have developed Raman diagnostic algorithm that is based on relative contribution of fit coefficients of fat and collagen. This algorithm was applied in a prospective manner, while DRS/IFS algorithm was developed using logistic regression. Figure 1 depicts the schematic representation of the study results.
The clinical studies demonstrated the potential of Raman and DRS/IFS spectroscopy as a clinical tool for diagnosis of breast cancer. Furthermore, we have applied our Raman spectroscopy technique to assess status of margins during lumpectomy/mastectomy surgical procedures. In fact, using our technique we were able to correctly identify the only one grossly invisible cancer, that was diagnosed as ductal carcinoma in situ (DCIS) upon histopathological evaluation. Had Raman spectroscopy been used in a real-time fashion to guide tissue excision during the surgical procedure, the additional reexcision surgery might have been avoided.
The future studies include development and evaluation of multimodal technique – the combination of Raman, DRS and IFS spectroscopy; as well as application of our technique to guide core needle biopsy in real time.
Publications:
1. “Diagnosing Breast Cancer Using Raman Spectroscopy”, Haka, AS, Shafer-Peltier, KE, Fitzmaurice, M, Crowe, J, Dasari, RR and Feld, MS. Proceedings of the National Academy of Sciences 102 (35), 12371-12376 (2005).
2. “In Vivo Margin Assessment During Partial Mastectomy Breast Surgery Using Raman Spectroscopy”, Haka, A, Volynskaya, Z, Gardecki, J, Nazemi, J, Lyons, J, Hicks, D, Fitzmaurice, M, Dasari, RR, and Feld, MS. Cancer Res. 66, 3317-3322 (2006).
3. “Diagnosing breast cancer using diffuse reflectance Spectroscopy and intrinsic fluorescence Spectroscopy”, Volynskaya, Z, Haka, A, Bechtel, K, Fitzmaurice, M, Shenk, R, Wang, N, Nazemi, J, Dasari, RR, and Feld, MS. Journal of Biomedical Optics 13 (2), 024012 (2008).
|
 |